In LinkHMS, the Patients tab allows doctors and nurses to access patient-specific data, including visit records, prescriptions, test results, vaccinations, diagnoses, and other relevant information. This guide provides step-by-step instructions for setting up and managing records within the Patient’s Profile, covering all relevant sections visible on the interface.
Opening the Patient Records
- Navigate to the Patients tab from the sidebar.
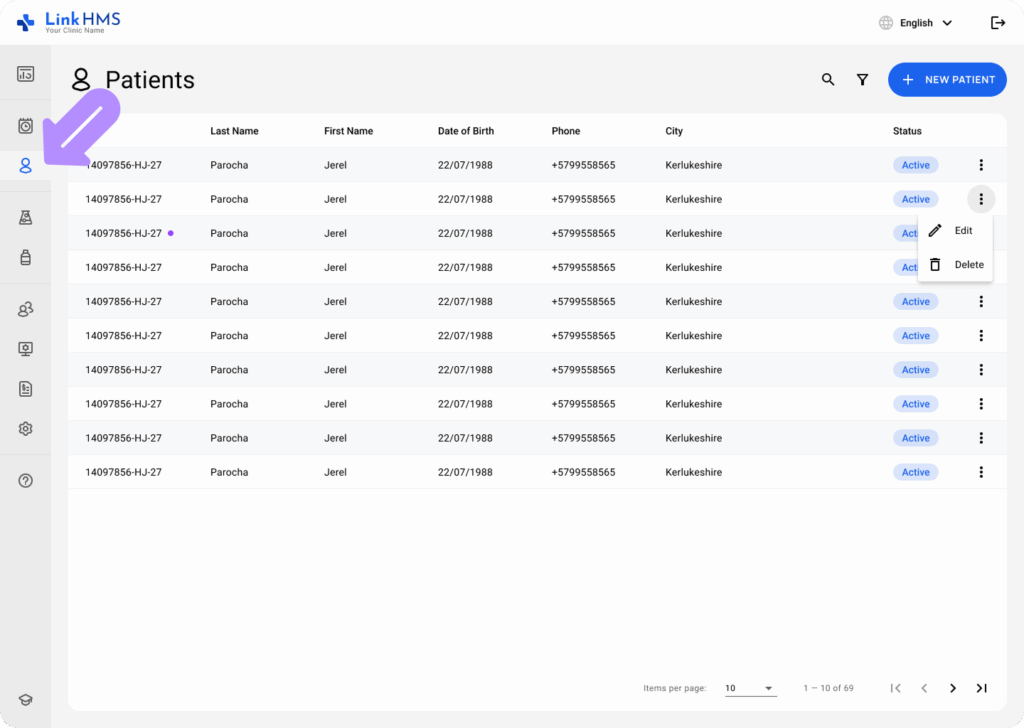
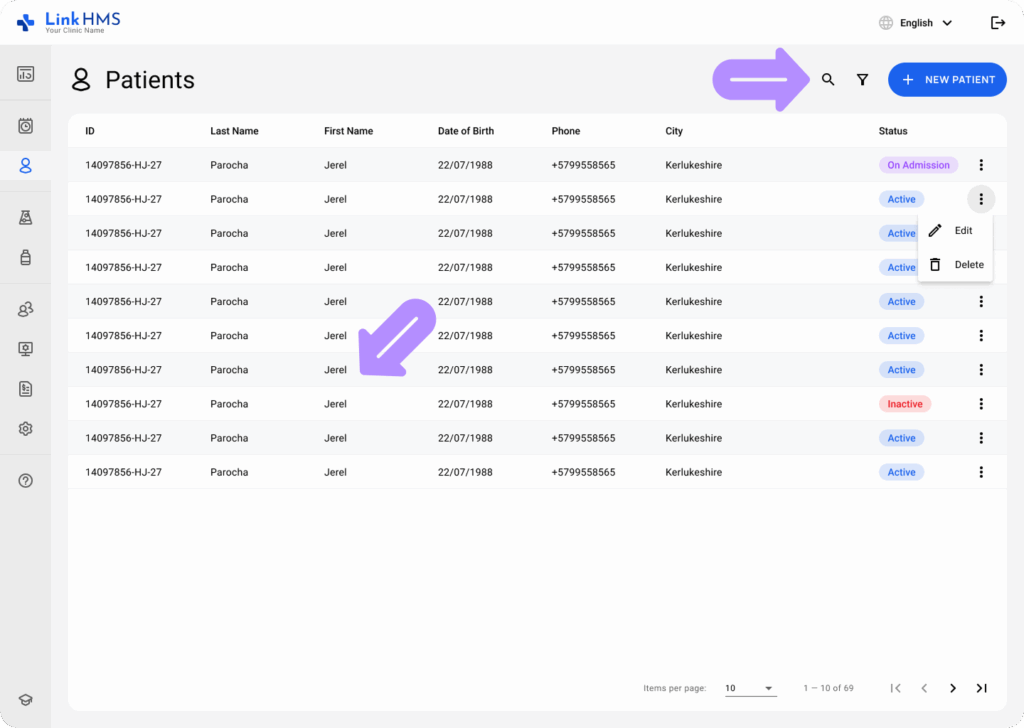
- Locate the required patient in the list. If needed, use the search bar or apply filters to narrow down the results.
Summary Section
The Summary section gives an overview of the patient’s recent visits, tests, prescriptions, and diagnoses. Here’s how to navigate this section:
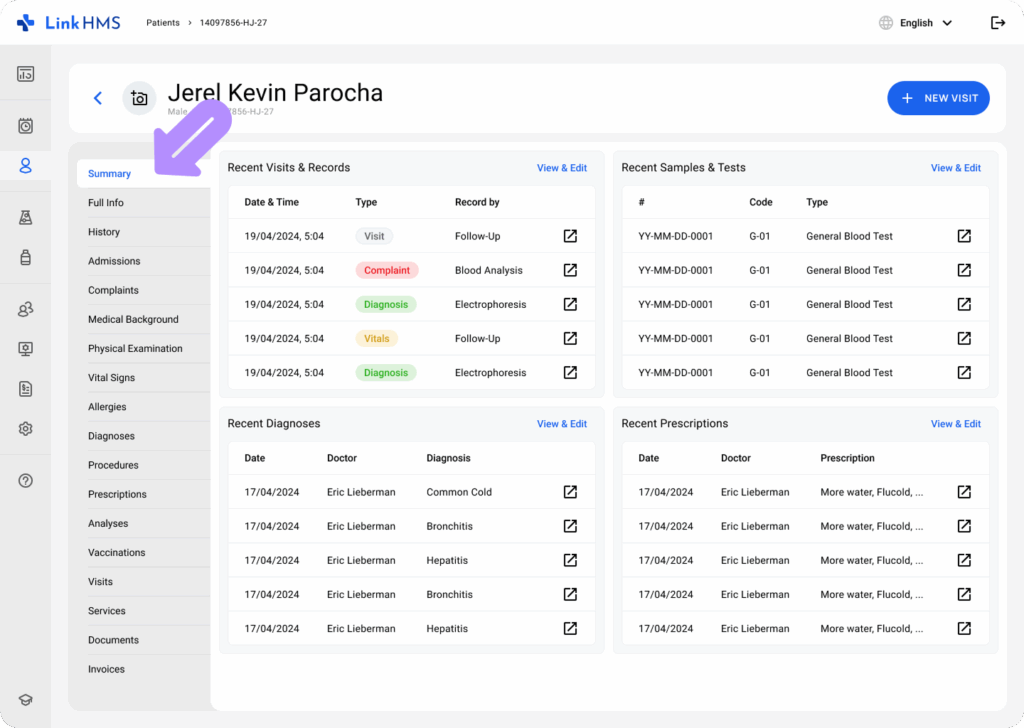
- Recent Visits & Records: Displays a list of the most recent activities, including date, time, visit type (e.g., appointment, analysis), and the recorder. You can click on the specific record to view full details.
- Recent Samples & Tests: Lists recent lab samples and different tests. The type and current status (To Do, In Progress, Waiting for Results, Done, Failed) of each test are visible. Click the icon next to the test for more details or to update the status.
- Recent Diagnoses: Displays diagnoses recorded by the doctor along with the date and relevant comments.
- Recent Prescriptions: Shows recent prescriptions written by the doctor, including medication, dosage, frequency, and total quantity prescribed.
Records Section
The Records section contains various categories where different aspects of the patient’s interactions and care can be documented. Here are the key categories:
- Full Info: Contains the patient’s name, general and medical info, contact information, emergency contact, and referrals. Authorized users can update this data if needed.
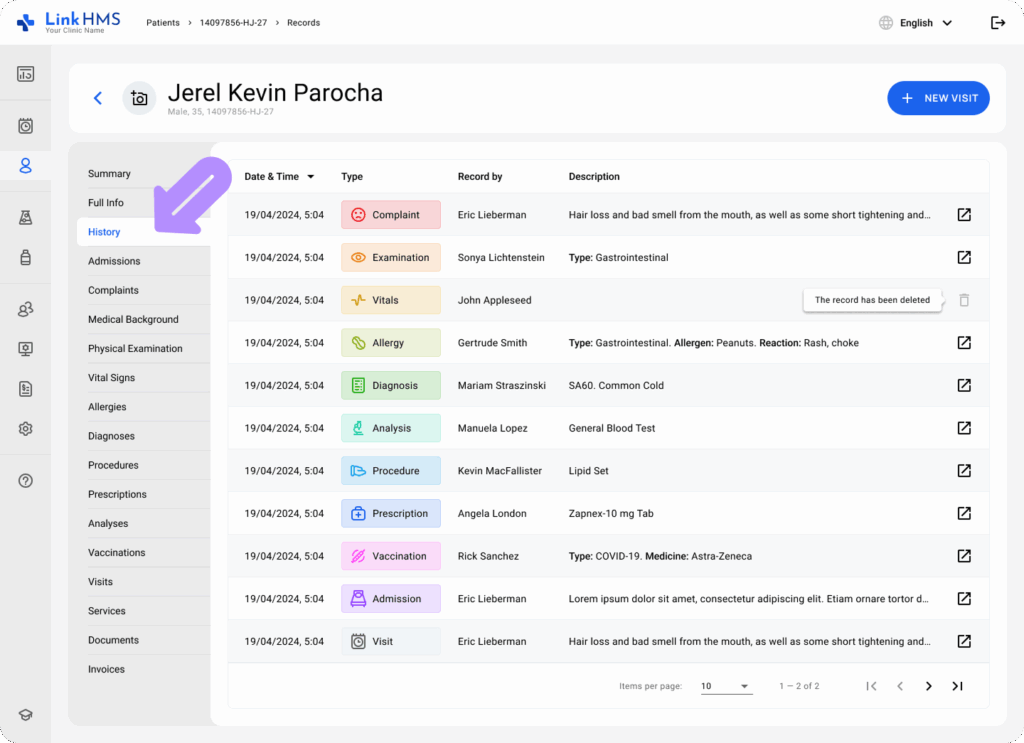
- History: Displays the full record of activities and interactions for providing patient care. It includes date & time, type, recorder, and description. You can preview more details for every listed record.
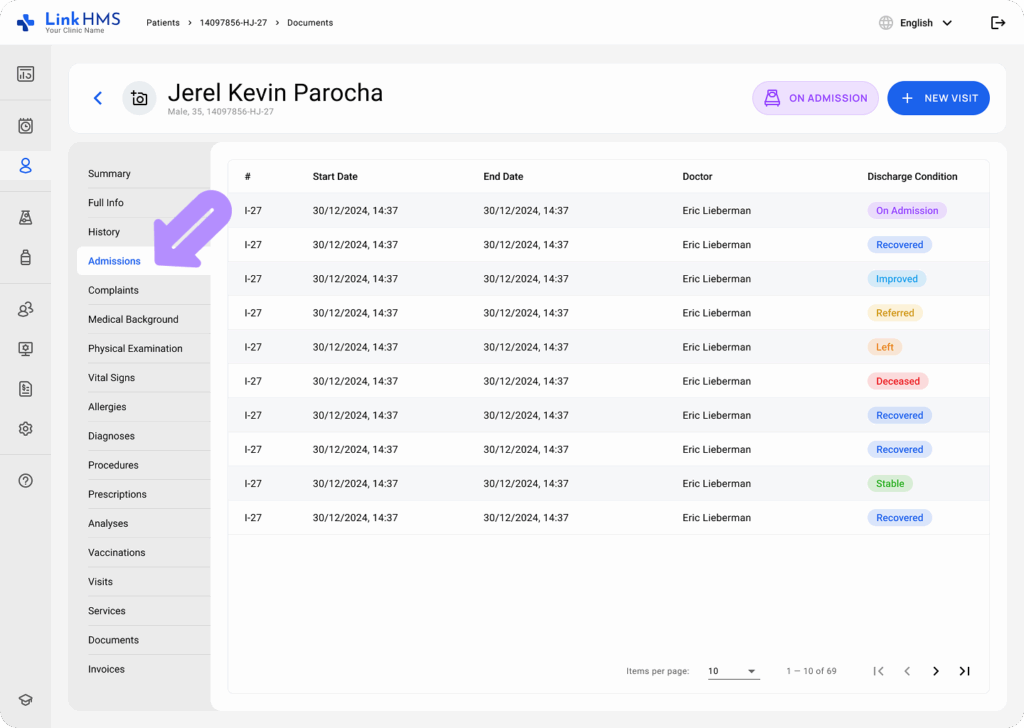
- Admissions: Lists active and past admissions with numbers, start and end dates, assigned doctors, and discharge conditions.
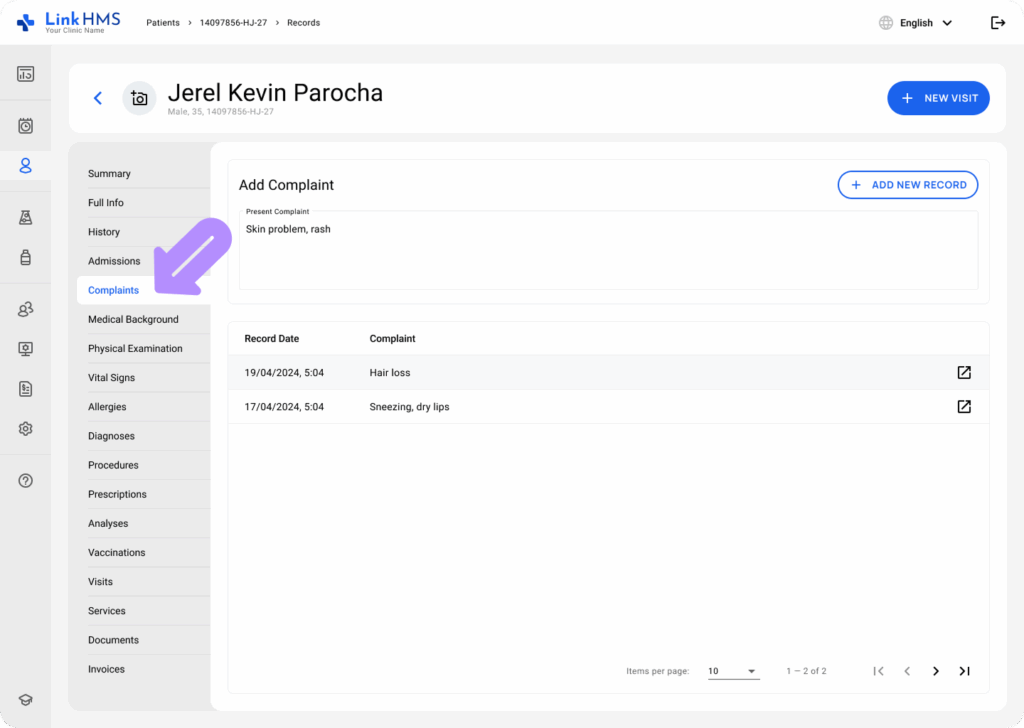
- Complaints: Provides a comprehensive history of the patient’s complaints, organized by date, that can also be updated by adding new ones.
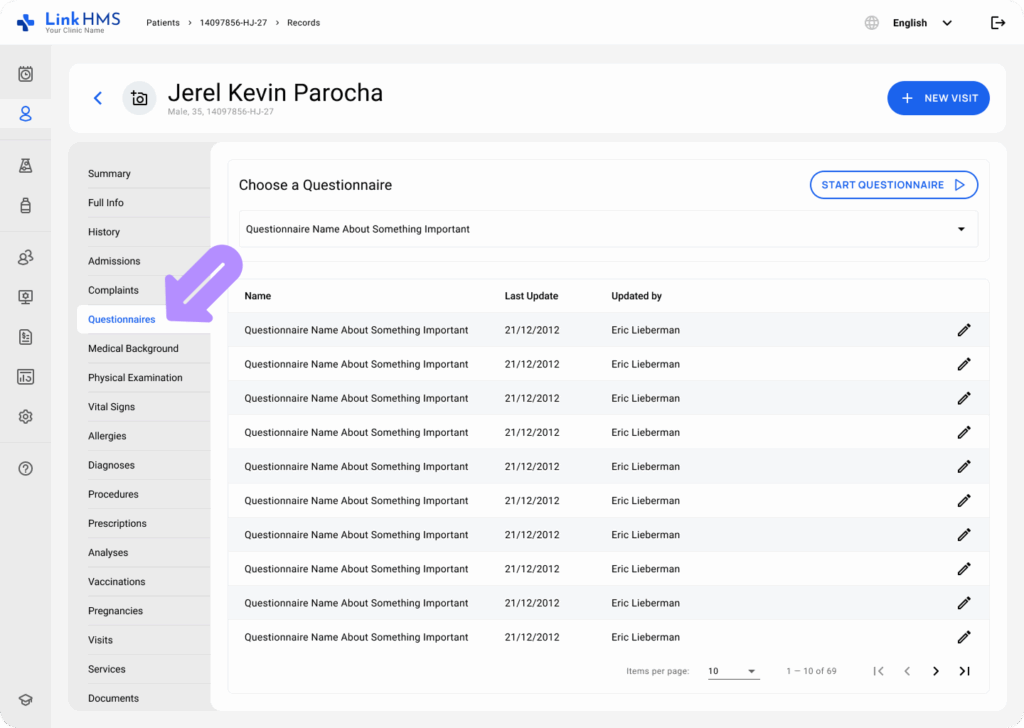
- Questionnaires: Displays a list of completed questionnaires and includes a button to start new ones.
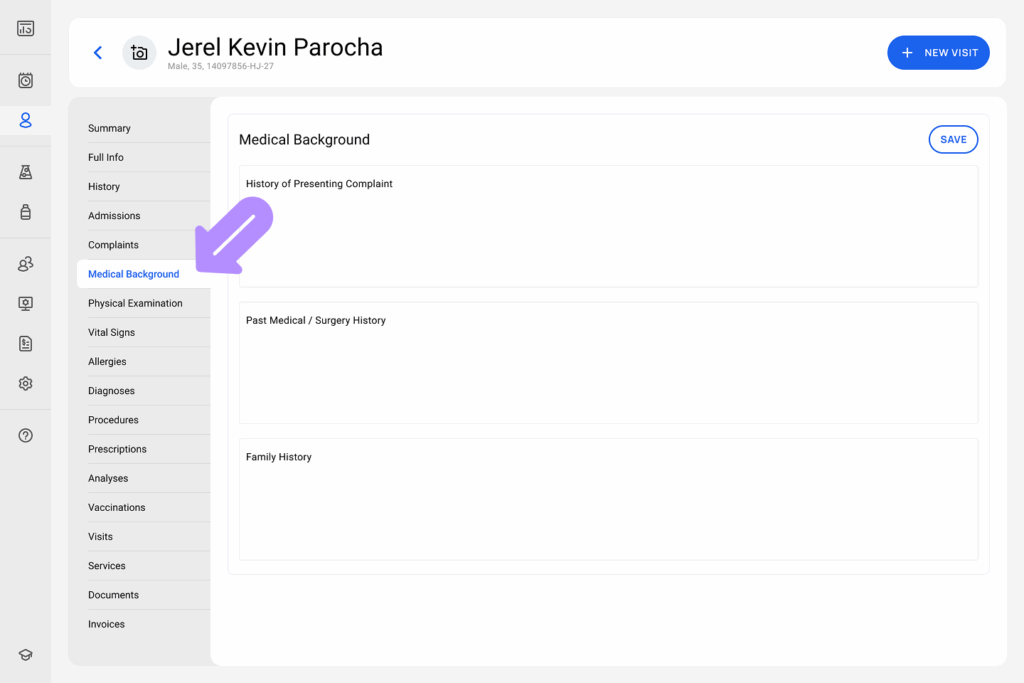
- Medical Background: Review and update the History of Presenting Complaint, Past Medical / Surgery History, and Family History.
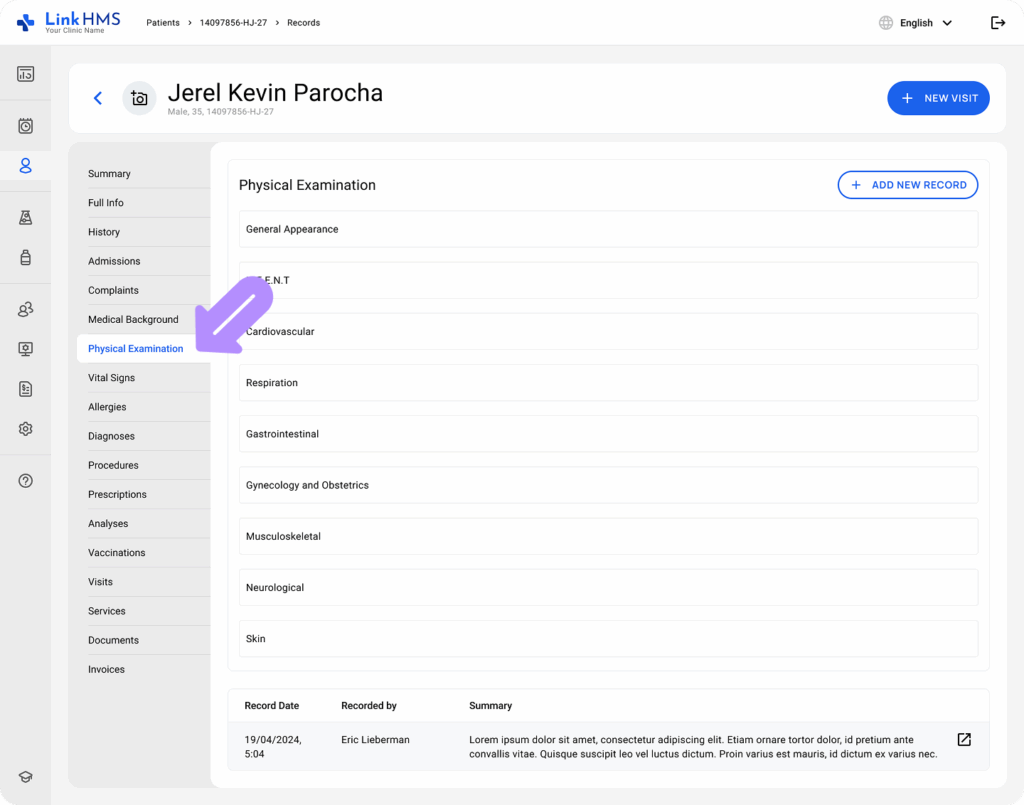
- Physical Examination: Presents the record of all the patient’s physical examination, including the record date, the recorder, and a summary. If required, users can add a new examination after filling in the listed field.
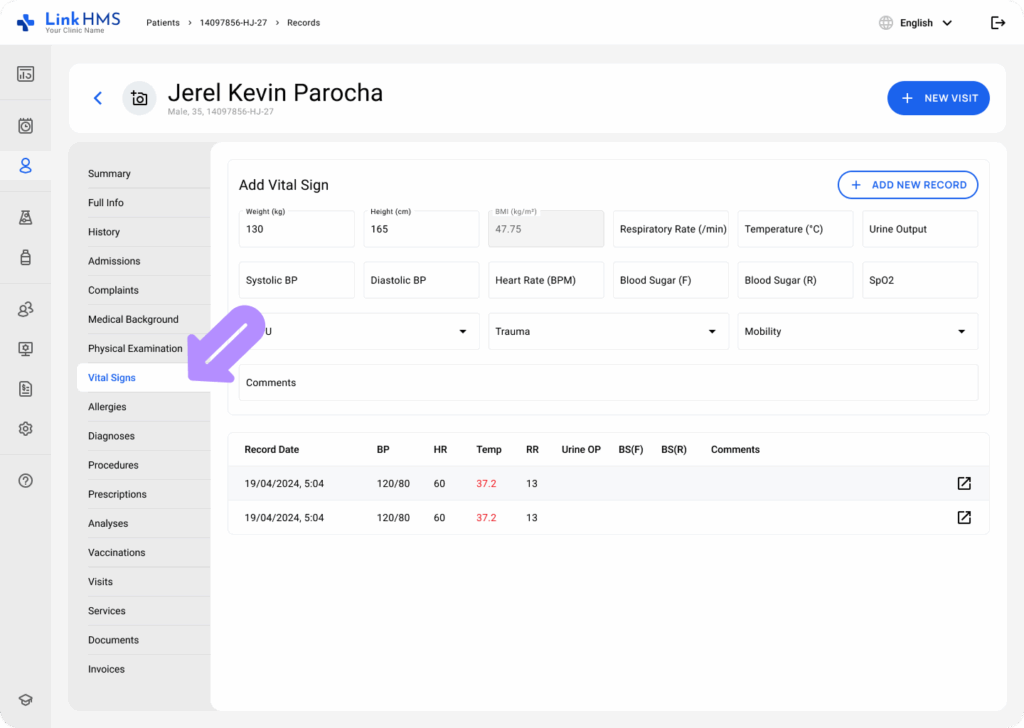
- Vital Signs: This section enables you to enter vital signs, including weight, blood pressure, respiratory rate, temperature, and other pertinent measurements. The vital signs are tracked for different dates, and any abnormal signs can be flagged.
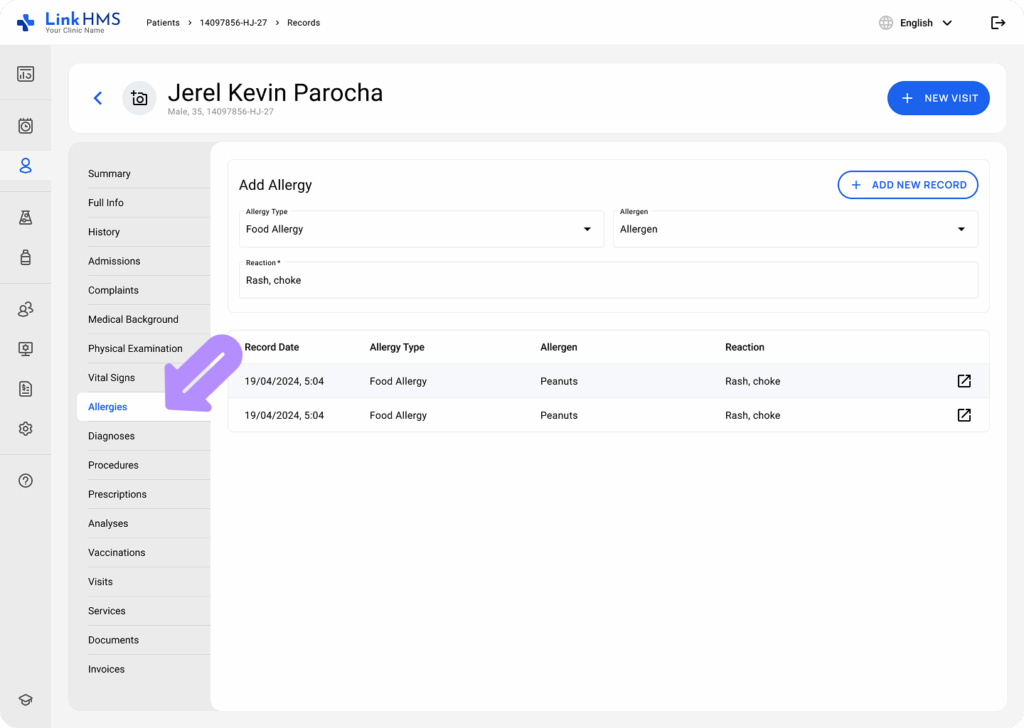
- Allergies: Lists patient allergies, the type of allergen, and the reaction. You can add, edit, or delete allergy records.
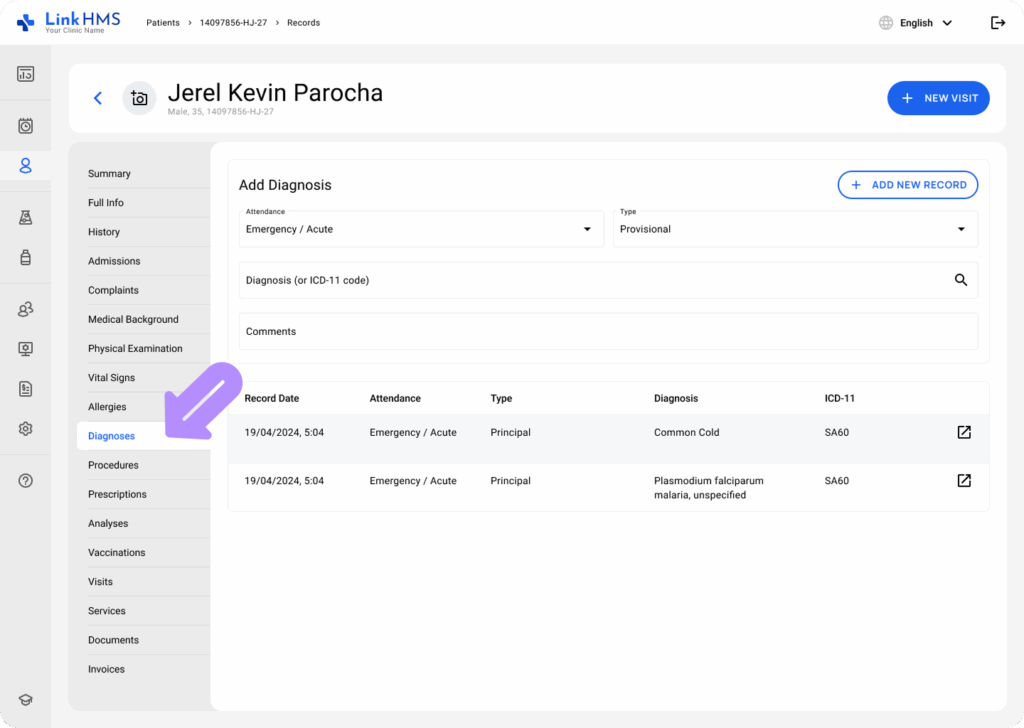
- Diagnoses: Records all diagnoses made for the patient. You can add new diagnoses and comments, and link them to the relevant ICD-11 codes for reference.
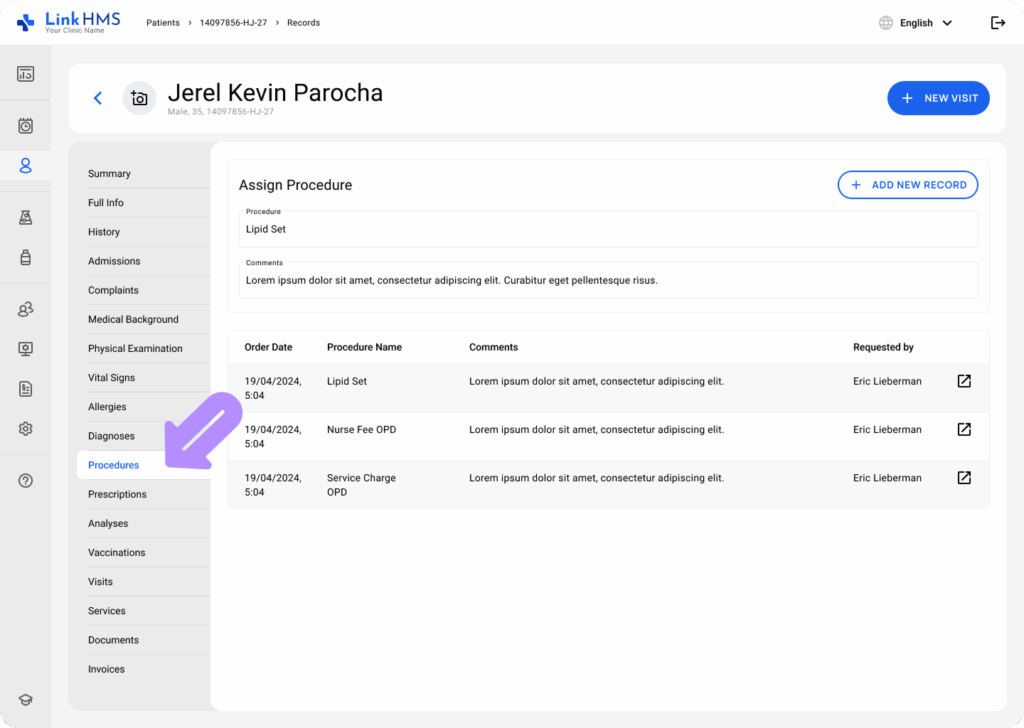
- Procedures: In this section, doctors can assign procedures (e.g., surgeries or tests). Each entry shows the procedure name, date, comments, and the practitioner who requested it.
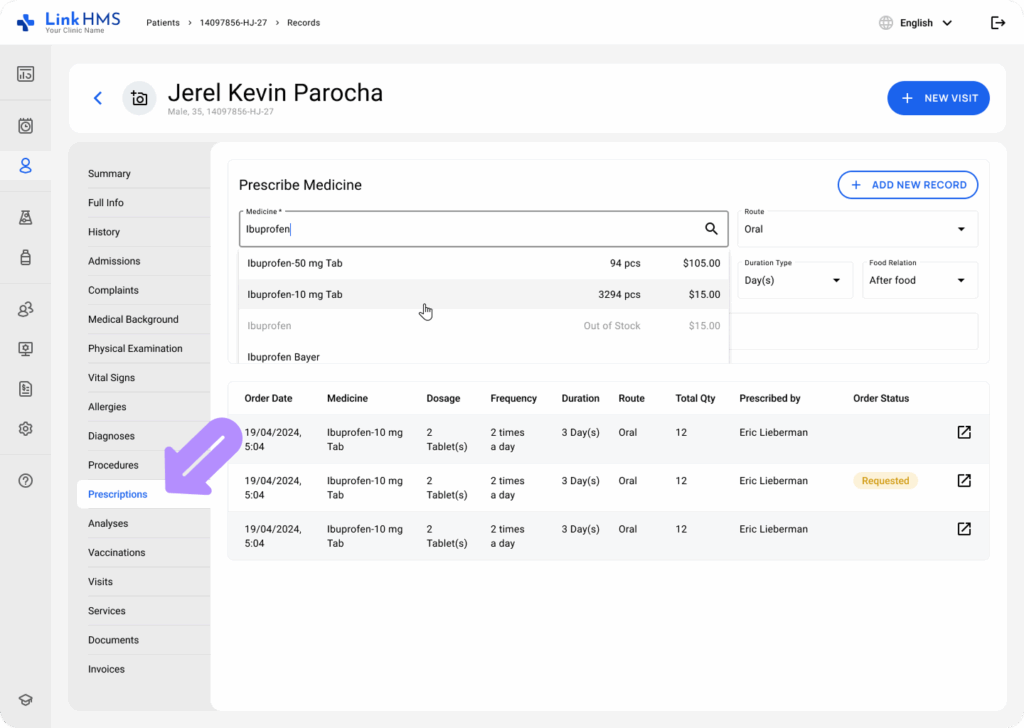
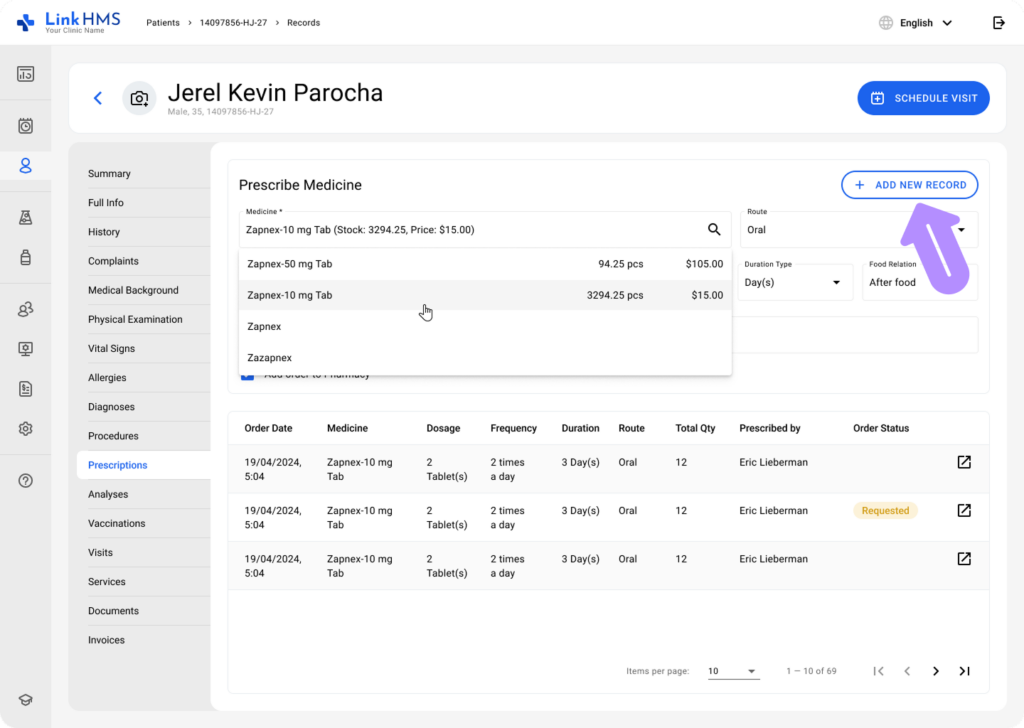
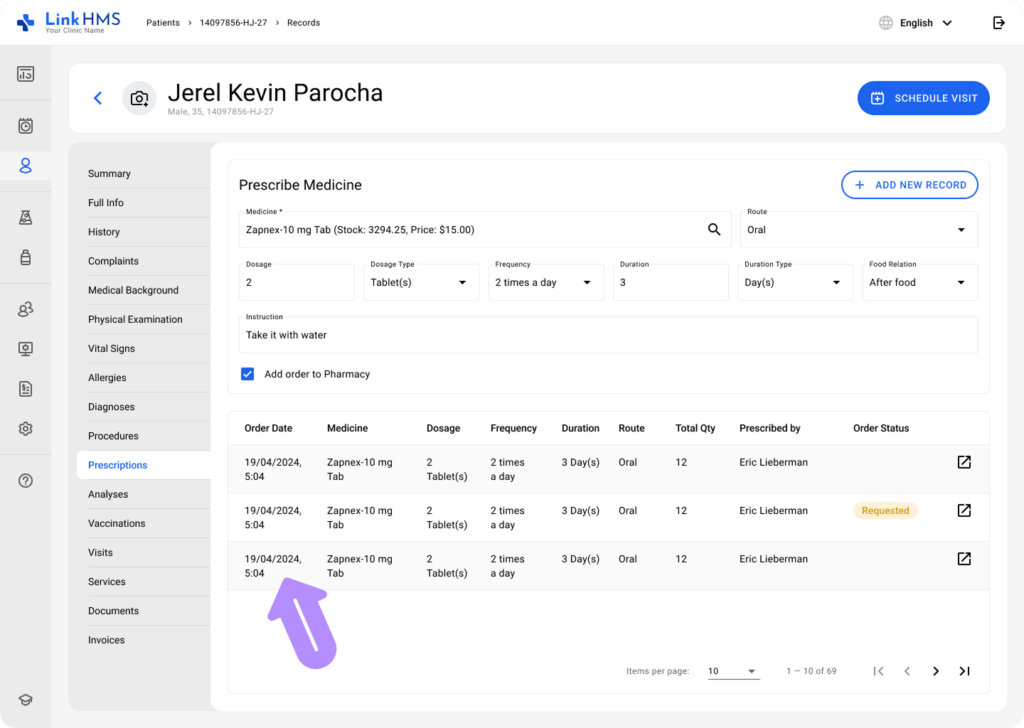
- Prescriptions: This section stores all prescribed medications, including the medicine name, dosage, frequency, route of administration, and order statuses. Doctors can add new prescriptions based on the available inventory stock and track past ones.
- Analyses: Lists all prescribed analyses or lab tests. The type of test (e.g., blood), its status (e.g., To Do or Failed), and price (when billable) are visible. New analyses can be instantly prescribed here.

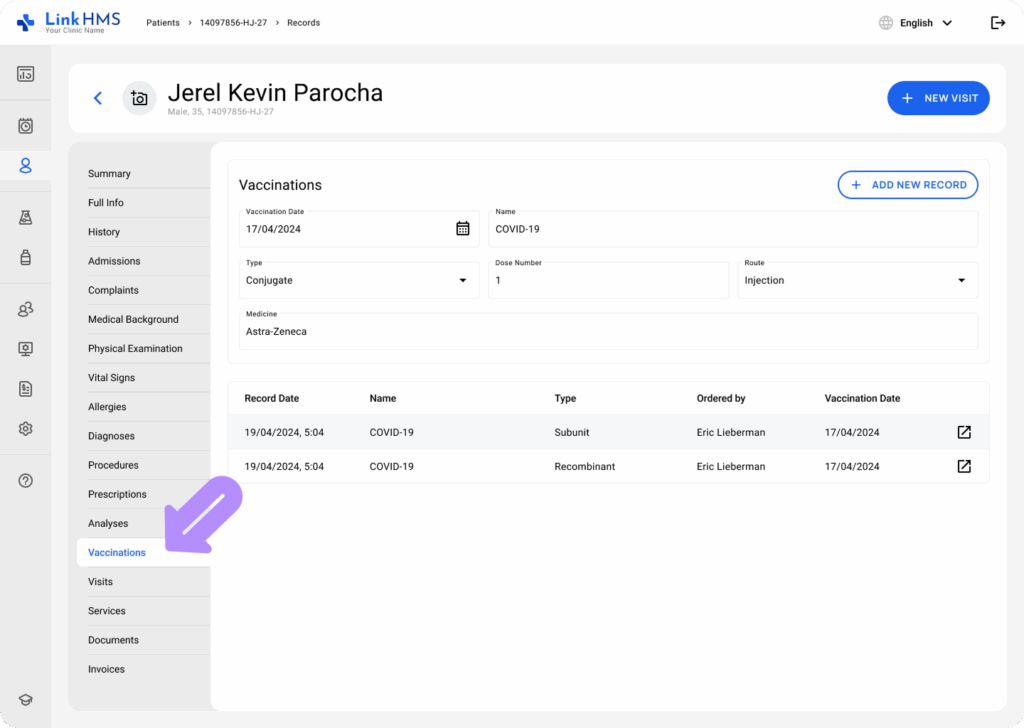
- Vaccinations: Displays the patient’s vaccination history, including details such as name, type of vaccination, dose, date administered, and the orderer.
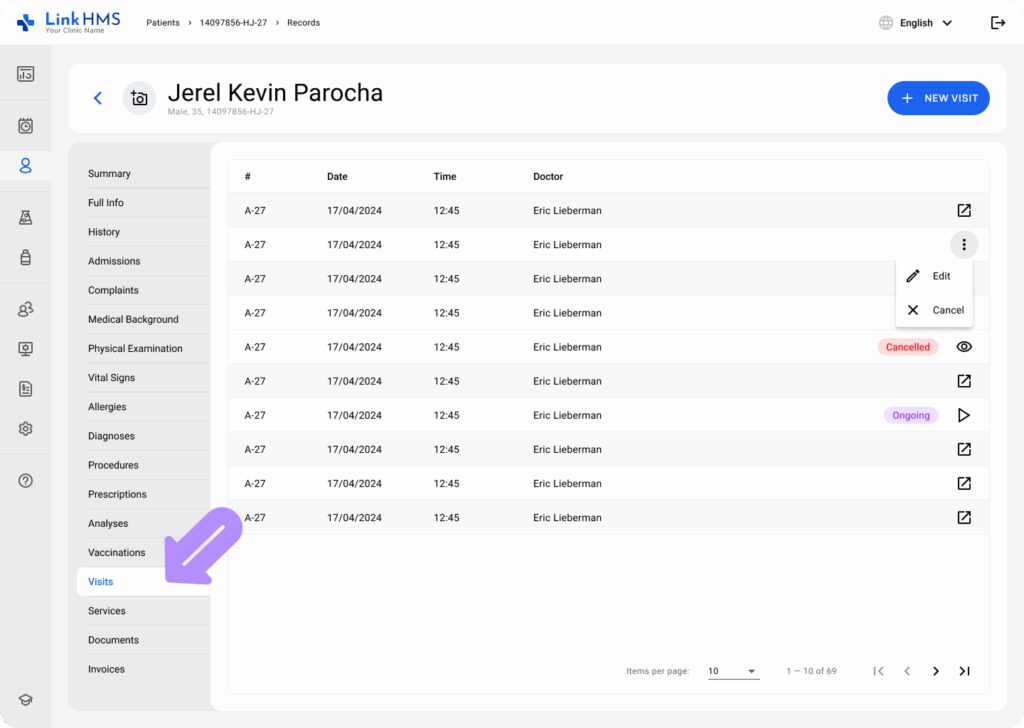
- Visits: Lists all scheduled visits, including the doctor’s name, date, time, and status (e.g., cancelled or ongoing). You can schedule or update visits here.
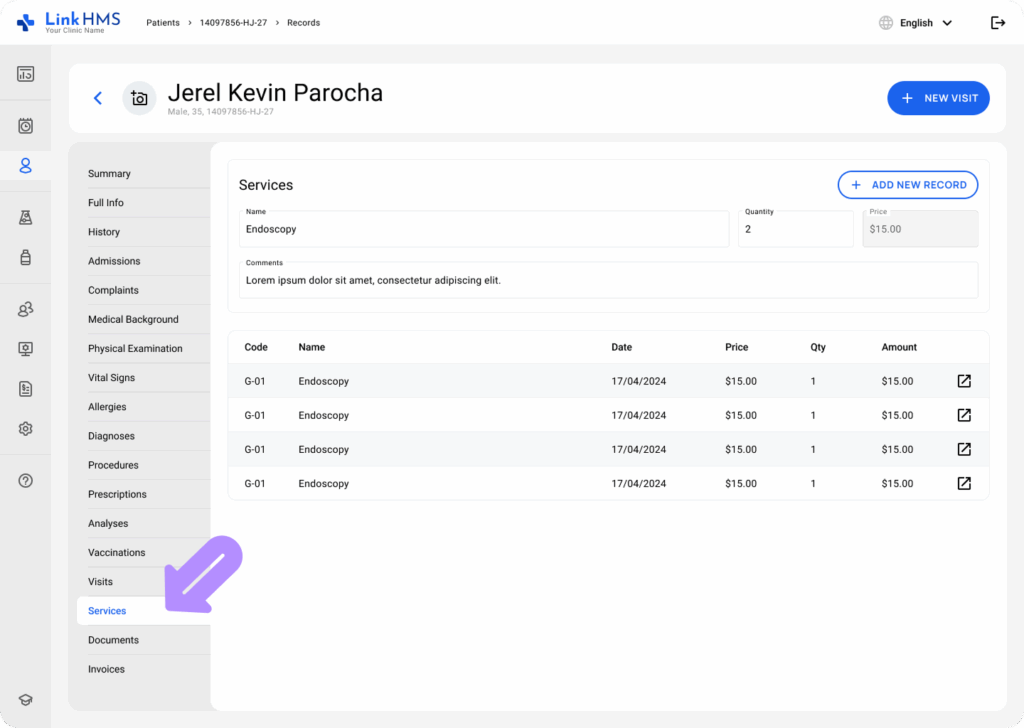
- Services: Contains a breakdown of all services provided to the patient. Each entry lists the service code and name, date, price, quantity, and total amount.
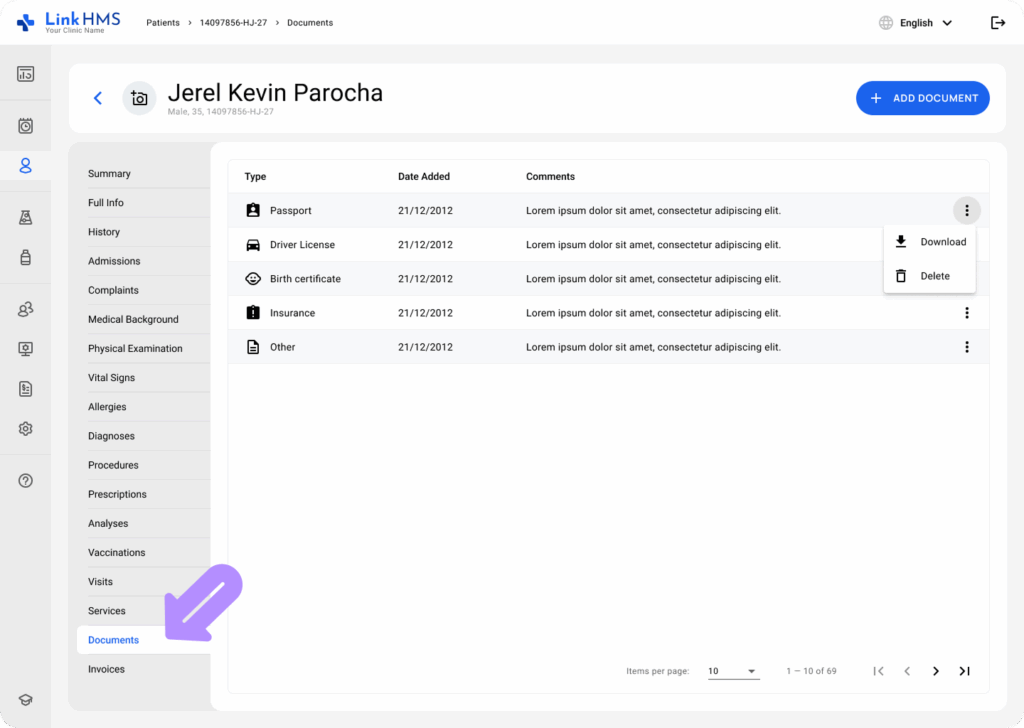
- Documents: Contains various types of patient documents, including the date added and optional comments. Authorised users can review and download the necessary documents.
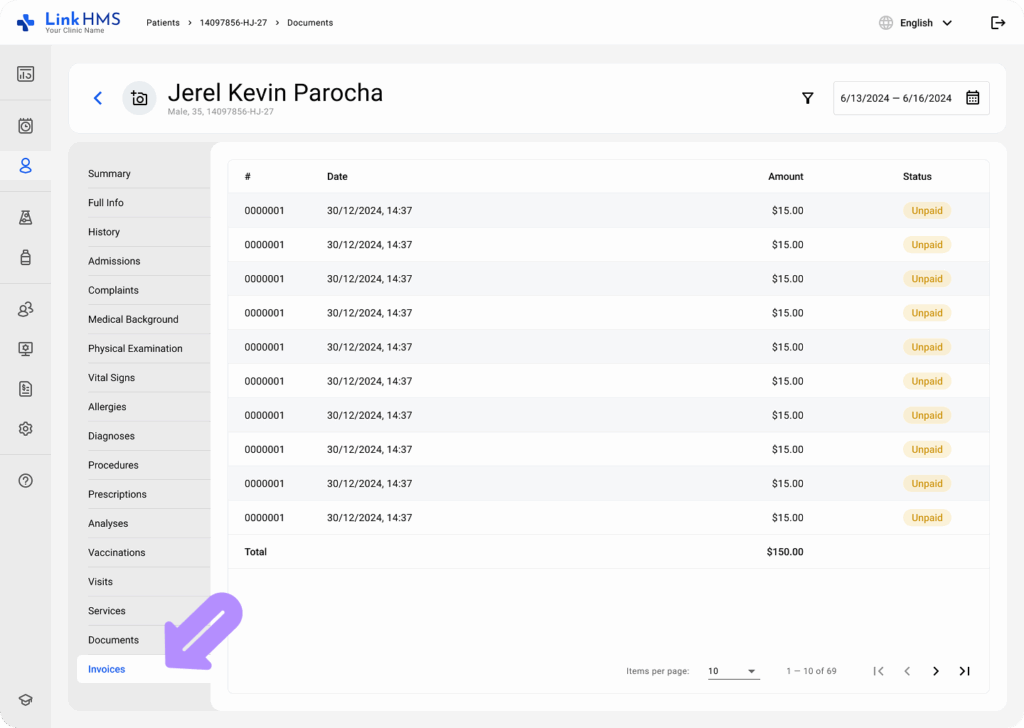
- Invoices: Displays a summary of all invoices associated with the patient. Each entry includes the invoice number, date, status, and the total amount charged. Users can filter invoices by date and navigate through records efficiently.
Interaction with Records
You can interact with each section by:
- Adding New Records: Use the + Add Record button available in each subsection (e.g., allergies, procedures, diagnoses, prescriptions) to input new information.
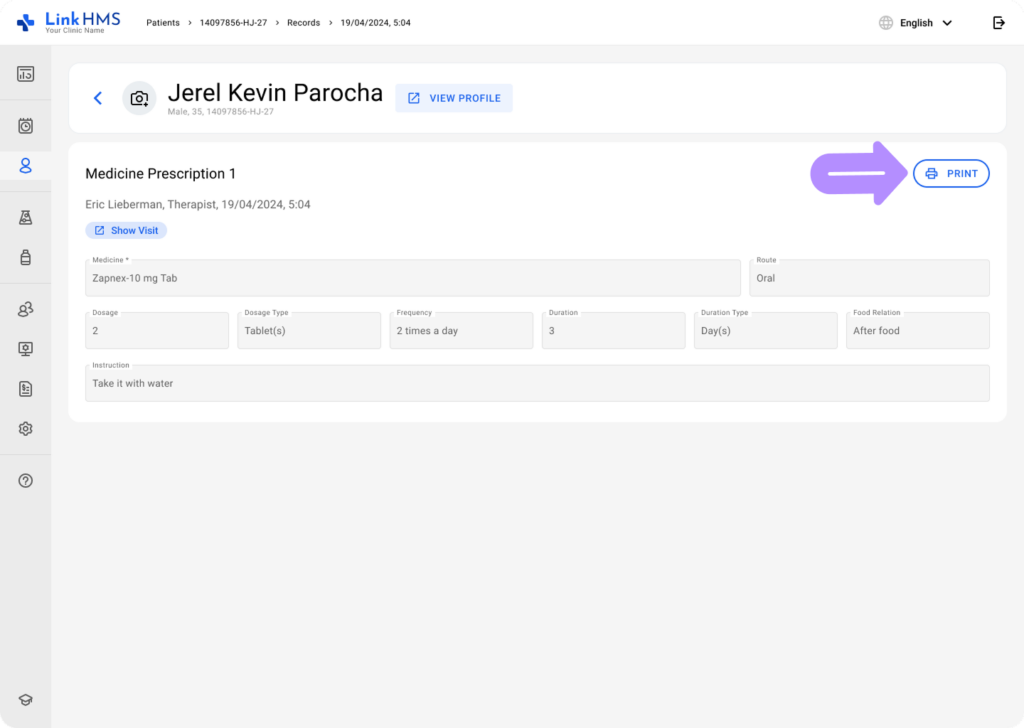
- Viewing Full Information: For each record, you can view the complete details by clicking the corresponding icon or text link.
Additional Functions
- Print Function: For some records, like analyses, visits, prescriptions, and others, the system offers a Print button to generate a printable document for easy sharing.
- Status Tracking: Many records, such as tests, prescriptions, visits, admissions, and invoices, are supplemented by the addition of the current status. These statuses help track the progress of each task or request, but can only be changed by authorised users.